
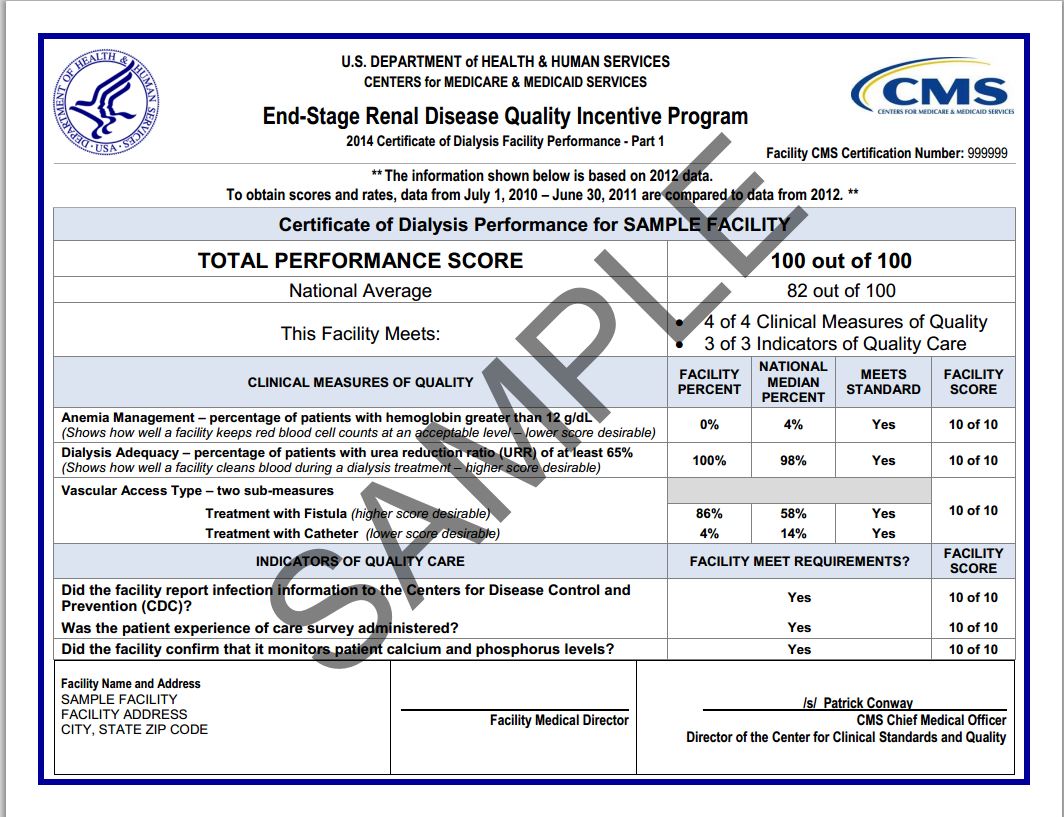
Last week, the Centers for Medicare and Medicaid Services (CMS) released its Proposed Rule specifying how dialysis facilities will be paid in 2015 and beyond. Most of the proposed changes relate to the Quality Improvement Program for dialysis. The Quality Improvement Program (QIP) sets performance standards for each clinic and penalizes clinics that do not meet or make progress toward the standards by cutting their payments by up to two percent. The purpose is to incentivize providers to do a better job by tying their pay to performance.
This year’s rule proposes several changes including new measures related to: patient experience, anemia management, and hospital readmissions rates. DPC’s annual patient survey asks your opinion on some of these issues. We hope to use your responses in writing our comments to CMS on the proposed rules. The survey is being conducted until July 31. You can make your voice heard by accessing the survey online or calling 1(888)-573-9026 and referencing project #14271.
Proposal 1: Patient Satisfaction Survey Results Will Count Toward QIP Payment Reductions
For several years now, dialysis facilities have administered the “CAHPS” survey to patients. However, under current regulations, dialysis facilities are only required to give the survey; poor results are not held against the facility in determining the payment. If the proposed rule is finalized, survey results would be tabulated and used to set payment.
In Medicare’s pay-for-performance system for hospitals, CAHPS survey results count toward bonuses and penalties. On the hospital side, observers have taken notice that hospitals are behaving much differently now that patient surveys affect their payment.
Counting the survey results could help to amplify the patients’ voice when giving feedback in their clinics.
Proposal 2: Anemia Management.
When the Quality Improvement Program for dialysis was first instituted, facilities were scored on how well they kept hemoglobin levels above a lower limit and how well they kept hemoglobin levels below an upper limit. The lower limit was eliminated after the labeling for Epogen was changed. This was of concern to patient advocates, because it appeared that after the lower limit was repealed, the number of transfusions dramatically increased.
As a result, the new rule proposes to monitor the transfusion ratio for each facility and penalize those facilities whose patients are disproportionately requiring transfusions. It would also repeal the upper limit, as patient hemoglobin levels rarely breach this current measure.
Proposal 3: Hospital Readmissions Rates
There has been a tremendous amount of policy activity in Washington, D.C. surrounding the issue of preventable hospitable readmissions. A “hospital readmission” occurs when a patient is discharged from the hospital and then comes back to the hospital within 30 days because of the same condition. Historically this happens in about 20 percent of Medicare patients and about 30 percent of dialysis patients. Medicare officials believe these rates are too high and so they have been penalizing hospitals with the highest rates. Along with the penalty there have been numerous other activities undertaken to improve patients’ transitions from the hospital back to the community.
The new rule proposes that dialysis facilities will also be penalized for hospital readmissions of their patients. This proposal is very controversial. The National Quality Forum is the multi-stakeholder organization that debates quality measures. There was significant division over whether dialysis facilities are in a good position to prevent readmission of their patients, because often they are not notified that a patient was in the hospital, nor given access to hospital medical records. By contrast, hospitals often have a staff member dedicated to discharge follow-up and can arrange appointments with the nephrologist when the patient is discharged.
Another factor in the mix is that the National Quality Forum is now recommending that readmission penalties account for patients’ socio-economic status. That recommendation is pending before Congress and will likely take years before a formula that adjusts for existing health disparities can be developed and agreed upon.
Medicare Dialysis Payment Rule: No Cuts for 2015!
One issue that patients will not have to worry about this time around is payment cuts to dialysis facilities. The base payment for 2015 will be the same as it is in 2014, due to a directive from Congress. That said the cost of care continues to increase, so even though payment remains the same, providers will be asked to do more with the same level of funding. At the same time, there are some adjustments to payment formula, increasing the weight accorded to labor costs (which vary geographically) and decreasing the weight accorded to drug costs (which are the same everywhere). This means that more of the overall dialysis budget will be directed to facilities in regions with a high cost of living, and less to areas with a low cost of living. This is expected to reduce payments to rural facilities by a little over one percent. DPC will be evaluating the effect that this could have on patient access in areas with low population density, while encouraging CMS to consider an unintended consequences.






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}